
If you like these cartoons, please support them! A $2 pledge really helps.
Even for chronic pain patients who aren’t mistaken for drug-seekers, the possibility that they might be is always lurking. It can color all of a patient’s interactions with care providers. For patients, the stakes are ludicrously high, and the fear of being seen as an addict and cut off from pain medication makes many patients’ already terrible situations worse.
From Brianna Ehley in Politico:
Last August, Jon Fowlkes told his wife he planned to kill himself.
The former law enforcement officer was in constant pain after his doctor had abruptly cut off the twice-a-day OxyContin that had helped him endure excruciating back pain from a motorcycle crash almost two decades ago that had left him nearly paralyzed despite multiple surgeries.
“I came into the office one day and he said, ‘You have to find another doctor. You can’t come here anymore,’” Fowlkes, 58, recalled. The doctor gave him one last prescription and sent him away.
Like many Americans with chronic, disabling pain, Fowlkes felt angry and betrayed as state and federal regulators, starting in the Obama years and intensifying under President Donald Trump, cracked down on opioid prescribing to reduce the toll of overdose deaths. Hundreds of patients responding to a POLITICO reader survey told similar stories of being suddenly refused prescriptions for medications they’d relied on for years — sometimes just to get out of bed in the morning — and left to suffer untreated pain on top of withdrawal symptoms like vomiting and insomnia.
The opioid crackdown was intended to cut down deaths from opioid overdoses. But legally prescribed opioids aren’t behind the vast majority of opioid deaths. Researchers in The Journal of Pain Research found that “fewer than 10% of opioid-related deaths involved prescription pain relievers without… other dangerous substances [such as heroin and fentanyl].”
It would be reasonable to expect that the increasing prevalence of heroin and illicit fentanyl in drug-related deaths would encourage policymakers to thoughtfully reconsider the relationship between opioid prescribing and deaths involving opioids. The data suggest that the overdose crisis is largely an unintended consequence of drug prohibition. Prohibition provides powerful economic incentives for illicit manufacturers, transporters, and dealers to supply banned substances. Nonmedical users appeared to prefer diverted prescription opioids, perhaps because the doses were reliable or because the fact that they could be legally prescribed for medical purposes created the illusion that they were relatively safe. But as diverted pain pills became more difficult to obtain in recent years, the black market filled the void with cheaper (and more dangerous) heroin and illicit fentanyl. …
Ending drug prohibition will not curb the growing tendency to use drugs nonmedically. However, it will potentially reduce the resulting harm…. Health care in general, and pain and addiction management in particular, are nuanced undertakings. Current public policies aimed at reducing opioid-related deaths ignore such nuance in favor of ham-handed, empirically dubious, and demonstrably harmful dictates. Americans suffering from chronic pain, and those from whom they receive their treatment, deserve medical care managed through better-informed and more even-handed policy.
Some readers will – quite reasonably – object to how this cartoon villainizes a doctor. Doctors, after all, didn’t crack down on pain medications out of nowhere. Doctors were (and are) reacting to public policy, and the fear of unreasonable regulators yanking their licenses. And I did consider incorporating that information into this cartoon.
But I couldn’t find a way to incorporate all of that without sinking the cartoon under the weight of too much exposition. And many pain patients have reported dealing with medical providers (not always doctors) who seem obsessed with finding any sign of drug-seekers, to the point of making legitimate pain patients feel like suspected criminals.
In the end, I decided this cartoon should take the perspective of pain patients, not the perspective of doctors. I wanted the cartoon to focus on the catch-22 pain patients face, where virtually any response – and in particular, any response that involves the patient standing up for themselves – could be interpreted as a sign of drug-seeking.
If I do another cartoon on this subject I might try to find an approach that looks at the systematic and regulatory pressures on doctors to deliver sub-optimal care to pain patients.
One more quote, from Amanda Votta’s essay “How The Opioid Crackdown Is Hurting Chronic Pain Patients,” which I highly recommend if you have time for a medium-long read.
Politicians and policymakers are “using us as scapegoats in the opioid crisis,” Danielle said. Lynn, another of my informants, said: “They don’t want to deal with the fact that their drug war is a failure. People are still getting high. Blaming people like us for overdoses is easy because we’re dependent on opioids. We’re captive to the system, which, right now, feels like it’s trying to kill us by refusing to treat our pain.”
Drawing this one didn’t go smoothly. I expected panel three to be the really fun panel to draw, but when the time came I had trouble making the face work. I actually ended up completely erasing the lower half of the doctor’s face and redrawing, but I’m not sure the new drawing was any better. Here’s are the two versions side by side:

I didn’t like the mouth in the first version – to me, it seemed like it was floating on the face rather than being part of it. And the mouth doesn’t seem correctly centered – it’s sort of drifting to the left side of his face. But then, the redrawn version doesn’t sit right with me either.
But eventually I had to stop redrawing and just be done. A completed “good enough” cartoon is always better than a cartoon that never gets finished because a drawing isn’t perfect.
I do like the figures in panel four – I like the way the patient is leaning way back from the doctor’s hostility, and I like the doctor’s sour expression and blank glasses for eyes.
TRANSCRIPT OF CARTOON
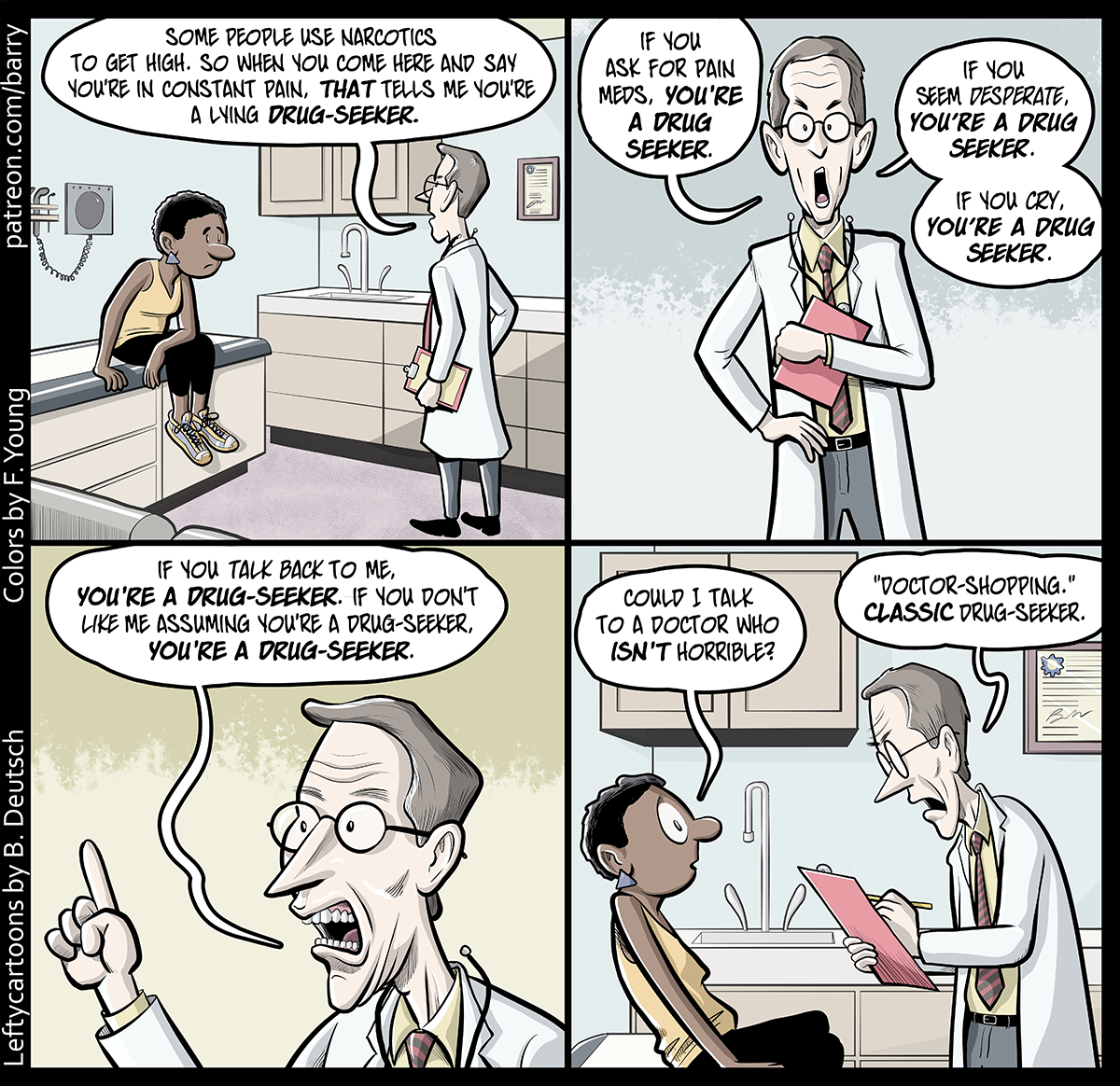
This cartoon has four panels. The cartoon is set in a doctor’s examining room – it has one of those tall examination tables with padding so patients can lie down, medical equipment and a degree hanging on walls, various cabinets, a sink. A tired-looking woman in a yellow tank top and black capri pants is sitting on the exam table. A doctor is standing in front of her. We can tell he’s a doctor because he’s wearing a white lab coat and has a stethoscope hanging around his neck. He’s holding a clipboard in one hand.
PANEL 1
The doctor is speaking to the patient. The patient is slumping a little, while the doctor is stiffly upright.
DOCTOR: Some people use narcotics to get high. So when you come here and say you’re in constant pain, that tells me you’re a lying drug-seeker.
PANEL 2
A closer shot of just the doctor as he speaks, looking stern and a bit angry, clutching the clipboard to near his chest.
DOCTOR: If you ask for pain meds, you’re a drug seeker.
DOCTOR: If you seem desperate, you’re a drug seeker.
DOCTOR: If you cry, you’re a drug-seeker.
PANEL 3
A close-up of the doctor’s face as he lectures, one forefinger raised.
DOCTOR: If you talk back to me, you’re a drug-seeker. If you don’t like me assuming you’re a drug-seeker, you’re a drug-seeker.
PANEL 4
A shot of the patient and doctor. The patient is now very wide-eyed, and leans back, away from the doctor. The doctor leans forward, hunching over his clipboard a bit as he makes a note.
PATIENT: Could I talk to a doctor who isn’t horrible?
DOCTOR: “Doctor-shopping.” Classic drug-seeker.
This cartoon on Patreon









 I drew this in an early stage of developing this white-on-brown style for cat drawings, and it was one of the pictures that encouraged me to continue because of the shock of recognition I felt when I looked “Pete” in the eye. It just really looks like him. I was also really excited by the way the paws turned out– the pattern of light shows the distribution of his weight in a way I don’t think I would have been able to capture without using a photograph as a template. He’s pondering a jump and his front paws are on the corner of a cabinet. I think getting that right helps the image feel like it’s arrested mid-motion instead of being a stiff pose.
I drew this in an early stage of developing this white-on-brown style for cat drawings, and it was one of the pictures that encouraged me to continue because of the shock of recognition I felt when I looked “Pete” in the eye. It just really looks like him. I was also really excited by the way the paws turned out– the pattern of light shows the distribution of his weight in a way I don’t think I would have been able to capture without using a photograph as a template. He’s pondering a jump and his front paws are on the corner of a cabinet. I think getting that right helps the image feel like it’s arrested mid-motion instead of being a stiff pose.



Don't forget that we built loopholes into our emissions and fuel economy regulations so car companies could get around the…